What Is Fascia? An Honest Guide to Why You Feel Stiff and Stuck
By Christopher "Chris" Clarke, Licensed Massage Therapist (FL MA #37417) — practicing since 2002. Last updated: May 29, 2026.

Fascia is the thin, tough sheet of connective tissue that wraps and connects every muscle, bone, organ, and nerve in your body — one continuous web from head to toe. Fascia tissue is mostly collagen, it's dense with nerve endings, and when it's healthy it glides. When it stops gliding, you feel tight, stiff, and "stuck."
That stuck feeling is real. What's causing it is almost never what the internet tells you.
I've spent twenty-four years with my hands on people's backs, necks, and shoulders. In that time I've watched fascia go from a tissue nobody mentioned to the thing every wellness page blames for everything — and sells you a gadget to fix. Most of what you'll read about it is half right and confidently oversold. So I'm going to do something different: tell you what fascia actually is, why your desk-bound body feels the way it does, and which of the popular "fascia fixes" the research supports versus the ones that are mostly marketing. Including the parts that aren't flattering to my own profession.
By the end you'll know what's really happening when you feel stuck, what genuinely helps, what to skip, and when stiffness is worth getting a doctor to look at. No hype. Just what I'd tell a friend on my table.
What fascia actually is — and why sources can't agree
Start with the simple version, because it's the part everyone gets right. Fascia is connective tissue, mostly collagen, arranged in sheets and wrappings throughout your entire body. Picture the thin white membrane you peel off a chicken breast, or the pith just under an orange's skin — that's fascia. It surrounds each muscle, bundles muscles into groups, lines your abdominal cavity, and sheaths your nerves and blood vessels. It isn't a set of separate parts; it's one connected system, which is exactly why a tight spot in one place can tug on somewhere else.
Now the part the other pages quietly disagree on. If you read three "what is fascia" articles, you'll get three different lists of the "types" of fascia. One says superficial, deep, visceral, and parietal. Another swaps in "meningeal." A third invents categories like "structural" and "spinal" that match neither of the first two. None of them mention that the others exist. The honest truth is that fascia researchers themselves don't have one tidy, agreed-upon classification — the tissue is continuous, so where you draw the lines is partly a judgment call. For your purposes, the useful split is just two: the superficial fascia right under your skin, and the deep fascia that wraps and separates your muscles. The deep layer is the part that tends to feel tight.
While we're clearing things up: you may have read that fascia holds "250 million nerve endings — more than your skin." It's a great line, and it's everywhere. It's also not a measured fact — it traces to a single researcher's back-of-the-envelope estimate that swings entirely on how broadly you define "fascia." What is well established, and what actually matters, is the next part.
Why your desk-bound body feels stiff and stuck
If you sit for a living, you know the feeling. The upper back that turns to concrete by 3 p.m. The neck that won't rotate the way it used to. The hips that feel welded after a long drive. You stretch, it loosens for ten minutes, then it creeps right back.
What's going on is glide. Fascia's layers are built to slide over one another, lubricated by a slippery substance called hyaluronan. Movement keeps that glide healthy; sustained stillness does the opposite. Hold the same posture for hours and the same tissues stay loaded the same way — and the system that's supposed to be moving and sensing settles into reporting one thing on a loop: tension.
Because fascia is one connected web, desk posture rarely stays put. The classic chain runs up the back of the body — tight calves and hamstrings from a seated day pull on the fascia of the low back, which pulls on the mid-back, which leaves you rubbing your neck. People come in convinced the problem is their neck, and the neck is just where they finally felt the bill for eight hours of sitting.
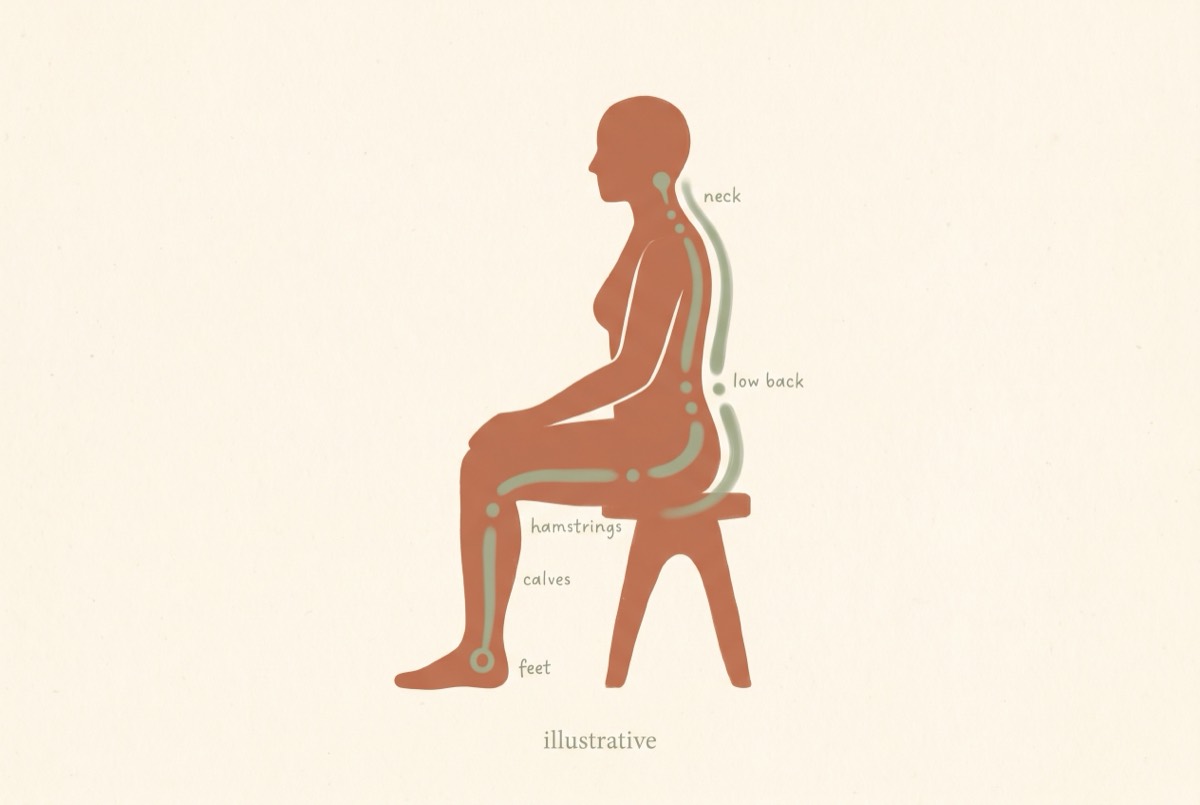 The desk-job load chain, foot to neck — illustrative.
The desk-job load chain, foot to neck — illustrative.
It's also why stretching alone disappoints you. A stretch feels good and buys you some range — but the research is clear that what's mostly changing is your tolerance to the stretch, not the length of the tissue. You didn't lengthen your fascia in thirty seconds. You turned the alarm down for a few minutes. Which raises the real question: what is that alarm, and who's pulling it?
A ten-second self-check. Sit tall and press your thumb into the muscle just beside your spine, up between the spine and the shoulder blade — on the muscle, never on the bone. If it's tender and a little ropey and you've spent the day at a desk, that's almost certainly guarded, under-moved fascia and muscle — not damage. An ache that eases as you breathe into it is the everyday kind. Sharp, shooting, or numb is the kind to get checked (more on that below).
Fascia is a sensor, not a knot to break
This is the reframe that changes how you treat your own body, so I'll plant the flag: fascia is one of the most richly sensory tissues you have. It's wired with nerve endings — that part of the popular story is true, even if the "250 million" number is shaky. Your deep fascia constantly reports load, stretch, pressure, and threat back to your nervous system. Good research has confirmed it carries genuine pain-sensing nerves, and that irritated fascia can throw a distinct, burning, hard-to-pin-down ache even when the muscle underneath is fine.
Sit with what that means. The "knot" you feel is probably not a literal tangle of tissue you need to physically break apart. It's far more likely a patch of fascia and muscle your nervous system has decided to guard — a spot where the alarm is stuck on. You're not a machine that needs forcing. You're a sensor network that needs reassuring.
That single shift explains why the dramatic "break up the knot" approaches so often disappoint, and why gentler things sometimes work better than they have any right to.
Why relief works — but isn't what you think
Now the honest mechanics, including the part my profession would rather skip.
When a good massage leaves you looser and out of pain, something real happened. But it almost certainly wasn't me physically melting, lengthening, or restructuring your fascia. Deep fascia is genuinely tough — a well-known biomechanical analysis found the force needed to meaningfully deform it is far beyond what any hand, elbow, or foam roller can deliver. If you can't deform it, you didn't "release" it in the structural sense the marketing implies.
So what does happen? The relief is your nervous system letting go. Skilled hands-on work turns down the threat signal, restores glide between the fascial layers, and calms the guarding — and there's even evidence that massage quiets inflammatory signaling at the cellular level. The result is true and worth a lot: less pain, more freedom of movement, a body that feels like yours again.
Here's the part most pages miss, and it's the reason the work matters rather than a reason to skip it. A session's real job is to make the rest possible. You can't load, train, or rebuild a body that's locked in alarm — it just guards harder and hurts more. Hands-on work opens the window: it quiets the guarding and restores enough glide that your own movement and gradual loading can finally take hold. Because here's the honest timeline — the lasting change, where the tissue itself adapts and gets more resilient, comes from consistent loading over weeks, not from any single hour on a table. So the two halves need each other: the table gets you unstuck; your own consistency keeps you there. One good session plus the right movement beats ten sessions of being bulldozed — and anyone promising to permanently fix your fascia in a single hour is overselling it.
The honest fascia ledger: what helps vs. what's oversold
You came here partly to know what's worth your time and money. So here it is, graded the way I'd grade it for a friend — based on what the research actually shows, not what sells gadgets.
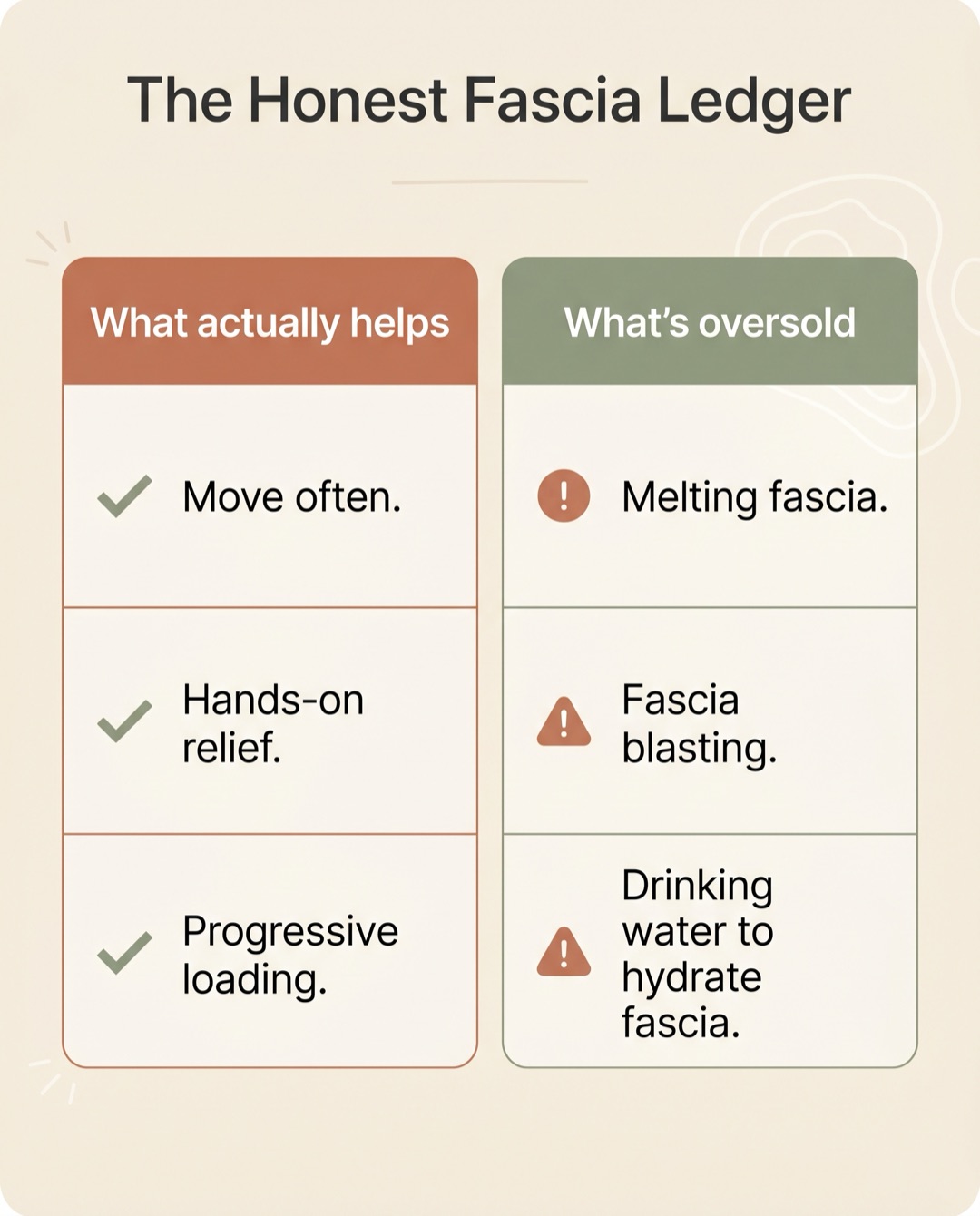 The honest ledger at a glance — full detail in the table below.
The honest ledger at a glance — full detail in the table below.
| The popular claim | The honest verdict |
|---|---|
| Movement & frequent posture breaks | Genuinely the best thing. Cheap, unglamorous, and more effective than anything dramatic. Glide depends on motion. |
| Hands-on bodywork for relief | Works — short-term and real. It calms the nervous system and restores glide; it's the reset that lets your own movement take hold, not a one-and-done cure. |
| Progressive loading / strengthening | The only proven route to durable change. Tissue remodels over weeks. This is the part that lasts. |
| Stretching | Good for comfort and range, not for "lengthening fascia." It raises your stretch tolerance; it doesn't restructure tissue, and it doesn't prevent injury (strength training does). |
| Foam rolling | Real, but brief. Solid acute range-of-motion gains with no downside — it works through your nervous system, not by "breaking up" anything, and it fades in 10–30 minutes. |
| Drinking water to "hydrate your fascia" | Not a thing. Your body controls your fascia's water, not your water bottle. Stay hydrated for real reasons — dehydration genuinely raises how much pain you feel — but you're not watering a plant. |
| The FasciaBlaster / "fascia blasting" for cellulite | Skip it. The evidence is weak and the cellulite claim isn't supported. |
| "We melt / realign / lengthen your fascia" | Marketing. You can't deform dense fascia by hand. The relief is real; that explanation isn't. |
If a page or a practitioner is selling you the bottom three as miracles, you've learned something useful about them.
Quick answers to the questions people actually ask
How do you release tight fascia? You don't "release" it the way the word implies — you can't physically unstick dense tissue by force. What works is calming the nervous system that's guarding it: gentle movement, warmth, slow controlled stretching to your comfortable edge, and hands-on work for a deeper reset. Then you keep the gain with regular motion.
What are the symptoms of tight fascia? A stiff, "stuck," or restricted feeling; achy areas that feel ropey or tender to press; reduced range of motion; tension that wanders (a tight spot in one place tugging on another). It usually tracks with how long you've been still and eases when you move.
How do you repair your fascia? For everyday desk stiffness there's nothing to "repair" — it's guarded, not damaged. You restore it by moving often, loading it gradually over weeks so it adapts, hydrating and sleeping well, and using hands-on work to reset stubborn areas. Genuine injuries are a different story and belong with a medical provider.
What does unhealthy fascia feel like? Persistently tight and sticky rather than supple; quick to stiffen when you're still; slow to loosen; sometimes a dull radiating ache. The tell is that movement helps and stillness hurts. Numbness, shooting pain, or pain that's worse at night is not "tight fascia" — see the next section.
When stiffness is worth getting a doctor to check
Almost all everyday stiffness is the benign, mechanical, desk-life kind this page is about. But a few signs mean the problem isn't fascia and needs a medical look first — not a massage, not a roller, not wait-and-see. Get evaluated promptly if you have:
- Numbness, tingling, or weakness in an arm or leg, especially if it's spreading or worsening.
- Pain that shoots down a limb rather than staying local.
- Loss of bladder or bowel control, or numbness around the groin — treat that as an emergency.
- Fever with the pain, which can point to infection.
- Pain after a significant fall or accident, particularly if you're older.
- Unexplained weight loss, or pain that's severe, constant, and worse at night instead of easing with rest.
None of these are anything to feel silly about checking. They're simply how you rule out the rare-but-serious before treating the common-and-mechanical.
How we help — and what only you can do
If you're in the Tampa Bay area and the desk-life version of stiff and stuck is your story, this is exactly the work I do — and it's the fastest way to get unstuck. A session with me does two things at once: a proper myofascial-focused massage that calms the guarding and restores glide, and an honest assessment to make sure your stiffness is the muscular, fascial kind and not one of the red flags above. Most people walk out moving more freely the same day.
That reset is also what makes the lasting change possible. Once your body is out of alarm, your own movement can do its job — which is why I'll point you toward simple stretching and mobility work and corrective exercise to keep the gains between visits. For a body that tightens up from sitting, a few minutes of desk-side relief goes a long way too.
I'll also tell you the truth about frequency: for most desk-driven tension, a session to settle a flare and then maintenance every few weeks does more for you than a standing weekly slot does for my schedule. When you're ready, you can see what a visit costs or book a time directly. Come in stuck; leave moving.
Your body isn't broken — it's reporting
If you take one thing from this page, take this: the stiffness you feel is a signal, not damage. Fascia is a sensing, connecting, gliding tissue, and when it complains it's usually telling you that you've held still too long — not that something's torn. The fix isn't force. It's motion, the occasional reset from skilled hands, and the patience to let tissue adapt on its own timeline. Treat your fascia like the sensor it is — listen to it, move it, reassure it — and "stuck" stops being your default setting.
Medical disclaimer & sources
This article is for general educational purposes only. It is not medical advice and is not a substitute for professional diagnosis or treatment. Always consult a qualified healthcare provider about your specific situation. If you have any of the red-flag symptoms above, seek prompt medical care.
Sources:
- Tesarz J, et al. Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience, 2011. PubMed
- Chaudhry H, et al. Three-dimensional mathematical model for deformation of human fasciae in manual therapy. JAOA, 2008. PubMed
- Crane JD, et al. Massage therapy attenuates inflammatory signaling after exercise-induced muscle damage. Science Translational Medicine, 2012. PubMed
- Langevin HM, et al. Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskeletal Disorders, 2011. PubMed
- Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Physical Therapy, 2010. PubMed
- Fascia (overview), Cleveland Clinic
Links
Resolved at Editorial against the live bookamassagenow.com WP REST API (all internal URLs confirmed to exist).
Internal (bookamassagenow.com) — ISC-5, 8 live links (exceeds 5+)
- /author-christopher-clarke/ — author byline (E-E-A-T Person→Org) — used in byline
- /myofascial-release/ — S7 "myofascial-focused massage"
- /stretching-mobility-coach/ — S7 "stretching and mobility work"
- /corrective-exercise/ — S7 "corrective exercise"
- /office-chair-massage/ — S7 "desk-side relief"
- /pricing/ — S7 "what a visit costs"
- /booking/ — S7 CTA "book a time directly"
- (reserve: /swedish-relaxation-massage/, /deep-tissue-massage/, /integrated-orthopedic-massage/ available if more needed)
REMOVED the prior /blog/lower-back-pain-massage/ link — that sibling article is NOT published yet (mid-production) and the site has no /blog/ path; linking it would 404. Re-add once it's live.
External (high-authority) — ISC-6, 6 sources (exceeds 3+)
- PubMed/NIH — Tesarz 2011 (PMID 21839150) — fascia innervation (S3)
- PubMed/NIH — Chaudhry 2008 (PMID 18723456) — can't deform fascia by hand (S4)
- PubMed/NIH — Crane 2012 (PMID 22301554) — massage anti-inflammatory signaling (S4)
- PubMed/NIH — Langevin 2011 (PMID 21929806) — tissue remodels with load (S4)
- PubMed/NIH — Weppler & Magnusson 2010 (PMID 20360057) — stretch tolerance (S2/ledger)
- Cleveland Clinic — fascia overview (S1)
All 5 PMIDs verified live against PubMed during the evidence-research stage.